This study examines the impact of three provider incentive payments: the Affordable Care Act Primary Care Incentive (PCIP), the short-lived Physician Shortage Area payment, and the Health Professional Shortage Area incentive payment on the availability of primary care practitioners and primary care services.
The study focused on the Medicare PCIP which increased the number of Medicare primary care providers by an average of 2.8 per county. Also the number of primary care physicians with a bonus eligible specialty increased by about 10 percent. There were more PCIP eligible claims per provider for one type of claim: the 25-minute visit for established patients. This was especially true of allowed charges for the eligibility threshold. While there was no significant incentive payment impact on allowed charges for the full sample of providers, for those who were near the PCIP eligibility threshold in 2009, increased charges of about $5600 annually were found in response to the policy. The study also models a fourth incentive payment, the ACA provision that for the years 2013 and 2014 primary care physicians providing Medicaid services be paid at no less Medicare rates.
Paul Hogan, Brighita Negrusa, PhD, and Projesh Ghosh, PhD contributed to this report. We benefited greatly from discussions with members of our technical expert panel. We also gratefully acknowledge the input from Caroline Taplin, the ASPE Project Officer and her colleague, Donald Cox. This study was conducted by The Lewin Group under contract number HHSP23320095639WC, task order number HHSP23337019T, with the HHS’s Office of the Assistant Secretary for Planning and Evaluation. The authors take full responsibility for the accuracy of material presented herein. The views expressed are those of the authors and should not be attributed to ASPE or HHS.
In this study, funded by The Assistant Secretary for Planning and Evaluation (ASPE), we analyze the impact of three different health practitioner incentives on the supply of primary care services: (1) the Medicare primary care incentive payment (PCIP); (2) the physician shortage area (PSA) bonus; and (3) the health professional shortage area (HPSA) bonus. Section 5501(a) of The Affordable Care Act authorized a quarterly incentive payment program to augment the Medicare payment for primary care services when furnished by primary care practitioners beginning in 2011 and ending in 2015. Medicare has been paying a HPSA bonus since 1987. Initially, the HPSA bonus was paid to physicians providing care in rural geographic HPSAs; in 1991 it was extended to services provided by physicians in urban geographic HPSAs. Subsequently, section 413a of the Medicare Modernization Act put in place an additional 5 percent bonus payment for physicians practicing in PSAs. PSAs were those counties and rural zip codes in MSAs with the lowest physician to population ratios. The purpose of these incentives is to increase the supply of provider services, both in general and for evaluation and management (E&M) in particular. In the case of the PCIP, it is to increase the supply of primary care services in Medicare. In the case of the PSA and HPSA bonuses, it is to increase the supply of services in certain locations designated as underserved.
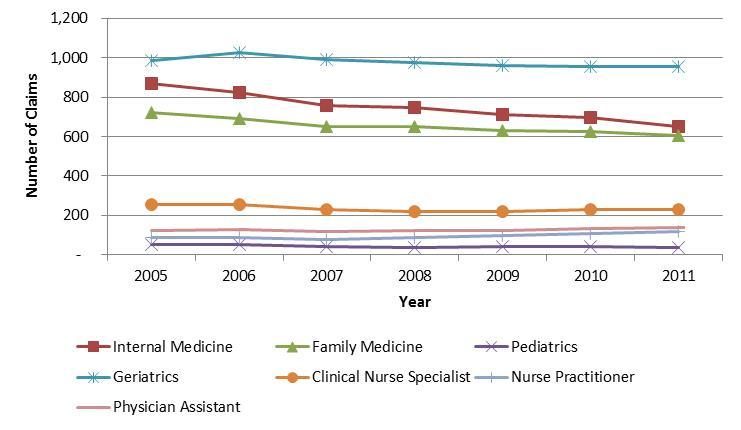
Volume of eligible claims submitted by the PCIP eligible providers and the impact of Medicare PCIP policy on the primary CARE services provided and other outcome measures of interest.
To explore these topics, we used a customized data set constructed at the provider level. This data set included all the claims submitted by the entire universe of Medicare providers each year from 2005 to 2011. Subsequently, each provider was linked by National Provider Identification number (NPI) to Provider360 data (available from Lewin Group’s parent company Optum Inc.) and the AMA Physician Master File to add provider characteristics such as provider demographics (e.g., age, gender), provider designation, medical school, and practice location. We also added geographic location-specific variables from the Area Resource File (ARF) based on the practice location information of providers. The main advantage of this pooled data set is the ability to track providers over time and capture changes in their volume of services in response to financial incentives.
We use a difference-in-difference (DID) approach to identify the effect of the financial incentives associated with the Medicare PCIP policy on key outcomes of interest. This method entails: (1) inclusion of a treatment group which is likely to be affected by the PCIP policy and a relevant comparison group not likely to be affected by the policy; (2) controls for year-specific effects common to both groups; and (3) an interaction of the treatment group and the year effects to capture the distinct impact of the policy on the treatment group. The model also controls for provider demographics and regional characteristics. One advantage of the DID estimation approach is that it enables us to disentangle the net impact of the 10 percent PCIP policy from changes that coincided with the PCIP policy affecting both the treatment and comparison group.
Policy makers have long been concerned about patient access to health care, particularly primary care, in underserved or shortage areas. We also focus on two additional financial incentive programs: Health Professionals Shortage Area (HPSA) bonus and Physician Shortage Area (PSA) bonus implemented in an attempt to improve access in shortage areas. These programs offer a higher rate of reimbursement in Medicare for eligible providers should they provide services in designated shortage areas. More specifically, we examine the following issues surrounding HPSA and PSA bonus:
Impact of PSA bonus on the number of primary care physicians and subsequent impact on the volume of primary care services.
Finally, we examine the existing evidence from the literature on the variation in Medicaid reimbursement rates relative to the Medicare rates to inform the impact of the Medicaid parity provision in the ACA. We describe the variation in Medicaid reimbursement rates relative to the Medicare rates, both for primary care and for all services, across US states during the period 2008-2012. Based on the empirical results from the PCIP analysis, we perform an exercise to simulate the effect of a 10 percent increase in the Medicaid-to-Medicare fee index on the proportion of US office-based physicians accepting new Medicaid patients across all states.
The estimated impact of the PCIP policy on the volume of primary care services, measured by the volume of claims, is somewhat mixed.
More specifically, there were more PCIP eligible E&M claims submitted per provider in a particular claim type: 25 minute office visits for established patients. Specifically, on average, there was a 7 percent increase in the number of 25 minute office visits claims due to the PCIP policy. Thus, the implied elasticity of the number of 25 minute office visits with respect to the incentive payment is about 0.7. Hence, it appears that the PCIP may have induced a substitution toward slightly longer visits for established patients.
For PCIP eligible E&M claims in general, the estimates from the DID model indicate that, on average, primary care providers with PCIP-eligible specialties submitted fewer claims (per provider per year) related to PCIP-eligible E&M services in response to the Medicare PCIP policy. 2 ,3
The positive impact of the PCIP bonus policy on the volume of E&M claims associated with 25 minute office visits for established patients is much stronger for providers near the PCIP eligibility threshold. 4 For the primary care providers near the PCIP eligibility threshold, there was almost a 15 percent increase in the number of claims for 25 minute visits due to the PCIP policy.
1 The increase in the number of physicians with a PCIP eligible specialty attributable to the policy is about 2 per county per year. This is almost 10 percent of the average number of primary care physicians in a given PCIP eligible specialty per county per year (average is almost 19). Therefore, given that PCIP policy provides 10 percent incentive payment, the implied elasticity of the number of physicians in PCIP eligible specialty with respect to the payment is about 1.
2 Not all primary care providers are eligible for Medicare primary care incentive payments. In summary, primary care physicians (with internal medicine, family practice, pediatrics and geriatrics specialty) who have at least 60 percent of the practitioner’s allowed charges under the Medicare physician fee schedule (excluding hospital inpatient care and emergency department visits) are for primary care services. The PCIP eligible primary care services are defined by specific E&M codes. Medicare PCIP is also provided to physician assistants, nurse practitioners and clinical nurse specialists who also meet the similar eligibility criteria.
3 Note that total eligible claims increased. Claims per provider declined potentially because additional providers were induced to submit eligible claims.
4 For the purpose of our analysis we consider the primary care physicians (with the PCIP eligible specialty) who have 50 percent-65 percent of their services for PCIP eligible E&M services (defined by specific E&M codes) to be near the eligibility threshold. We apply the similar method to select non-physicians (physician assistants, nurse practitioners and clinical nurse specialists) near the eligibility threshold.
5 The determination of the eligibility of providers in the first year (2011) of the PCIP is based on the extent of their PCIP eligible services in 2009. Besides, the announcement of the PCIP program was made in 2010. Thus, we assumed that the providers with Medicare PCIP eligible specialties would be potentially responsive to the PCIP program as early as year 2010 and alter their behavior. Subsequently, it is more meaningful to examine providers who were near the PCIP eligibility threshold in 2009 which is the year just before the policy effect is expected to influence.
6 Although the number of E&M claims went up due to the PSA bonus, it may be that within E&M services some services experienced an increase in allowed charges due to the PSA bonus while others experienced a decrease, accounting for the overall lack of impact.
7 Health Resource and Services Administration (HRSA) publishes Area Health Resource File (ARF) that includes HPSA status for each county within the US. For the purpose of our analysis we focus on primary care HPSA status. The ARF data classifies counties as full primary care HPSA if the whole county is considered as a HPSA.
The Affordable Care Act includes two key provisions regarding reimbursement to primary care providers ): (a) it provides a 10 percent incentive payment under the Medicare PCIP program to eligible providers (effective January 1, 2011); and (b) it raises the Medicaid primary care reimbursement rate at least up to 100 percent of the Medicare rate.
We find that as a result of the Medicare incentive payment the number of Medicare PCPs has increased on average by about 2.8 providers per county annually in 2010 and 2011. Also, the number of primary care physicians with PCIP eligible specialty increased by about 10 percent in response to the 10 percent incentive payment under the PCIP policy (i.e., elasticity of the number of primary care physicians with respect to the incentive payment is about 1). Eligible claims for some types of PCIP eligible E&M services and associated allowed charges have also increased. For example, on average, there was a 7 percent increase in the number of claims for 25 minute office visits due to the PCIP policy. On the other hand, in response to the PCIP policy, there was a 9.3 percent increase in the average allowed charges (for eligible services) among primary care providers with PCIP eligible specialties.
The reader should exercise some caution in interpreting these results, however. The behavioral response to the PCIP was observed in our data only for one year. The relatively short period may have resulted in insufficient time for a full provider behavioral response. In addition, the legislation provided for a program of only limited duration. Some providers may have chosen, explicitly or implicitly, not to change their behavior for a program of limited duration.
In addition, we find that Medicare providers were attracted to PSA areas through the PSA bonus, and submitted 7.8 percent more E&M claims annually during the PSA period. Gaining HPSA status also generated an additional 17 E&M claims submitted by primary care physicians with HPSA bonus-eligible specialties.
The reader is again encouraged to exercise some caution in interpreting the results for the PSA bonus. Because the criteria for the bonus include the actual supply of providers, there is a risk that the results may be biased. Though the methods we employ attempt to minimize the potential impact of this type of bias, we cannot be completely sure that the results are unaffected by this.
Finally, we document the variation in Medicaid reimbursement rates relative to the Medicare rates, both for primary care and for all services, across US states during the period 2008-2012, using the existing body of evidence. Using the empirical results from our PCIP analysis, we also perform an exercise to simulate the effect of a 10 percent increase in the Medicaid-to-Medicare fee index on the proportion of US office-based physicians accepting new Medicaid patients across all states. The simulation suggests that a 10 percent increase in Medicaid-to-Medicare fee ratio, would increase the US average of office-based primary care physicians accepting new Medicaid patients from 66.2 percent to 72.8 percent. Again, however, caution is warranted in a literal interpretation of this result, as it is based on an extrapolation from a different program.
The Assistant Secretary for Planning and Evaluation (ASPE) has contracted with The Lewin Group to examine the role of physician bonus and supplemental payment programs in increasing the supply of primary care providers (PCP) and the access of patients to their services.
The Congressional Budget Office has estimated that the implementation of the Patient Protection and Affordable Care Act (ACA) of 2010 will increase the number of nonelderly people who have health insurance—by about 13 million in 2014, 20 million in 2015, and 25 million in each of the subsequent years through 2024 (CBO, 2014). 8 Because those with insurance typically use more services than those without insurance, this increase in coverage will most likely result in additional pressure on a health care delivery system. 9 To address concerns about maintaining an adequate supply and distribution of primary care services, the ACA includes provisions that provide temporary financial incentives to primary care providers:
The Medicare primary care incentive payment is available to the eligible primary care practitioners for services provided under selected categories of E&M codes. An eligible primary care practitioner is a physician, nurse practitioner, clinical nurse specialist or physician assistant who satisfies the following criteria: (i) enrolled in Medicare with primary specialty designation of family practice, internal medicine, pediatrics and geriatrics; and (ii) at least 60 percent of the practitioner’s allowed charges are for primary care services. 10 This temporary 10 percent incentive payment is made on a quarterly basis. PCIP recipients with a family medicine Medicare specialty designation received an average incentive payment of $3,450 ($212,987,540/ 61,728) during the first year of the program. 11 This payment is equivalent to a two percent ($3,450/$201,512) increase in annual income. 12
In addition, Medicaid payment rates for primary care services delivered by primary care physicians must be no less than Medicare rates for the same services in 2013 and 2014. 13 Given the variability of Medicaid payments across states, this could be a substantial boost in payments for physicians in some states and less so in others. Medicare has been providing bonus payments to physicians in designated shortage areas to make these areas more attractive for physician practices. The Health Professional Shortage Area (HPSA) bonus and the Physician Shortage Area (PSA) bonus are specifically intended to address the geographic distribution of physicians.
The main purpose of this report is to present the key findings from our examination of the proposed research questions, the main data sources used for the empirical analysis, the methodologies used to identify the impact of payment incentives and detailed discussion of our analytical findings.
The report covers the three main categories of the empirical analysis:
A substantial portion of the empirical undertaking entailed analyzing existing Medicare claims data to understand the magnitude of these supplemental payments under Medicare and to estimate their impact on the supply of PCPs and their services. In this report we provide a detailed description of the data we use, our analytical approach and a thorough discussion of our analytical findings. The discussion in the report is organized as follows: section II presents findings from the review of relevant existing literature; in section III, we lay out the empirical methodology and main evidence related to the impact of the Medicare 10 percent primary care incentive payment; section IV describes the empirical analysis of the HPSA and PSA bonuses; section V presents the findings regarding the impact of higher primary care physician fees under Medicaid; finally, section VI is the conclusion.
9 Manning WG, Newhouse JP, Duan N, Keeler EB, Benjamin B, Liebowitz A, et al. (1988). Health insurance and the demand for medical care. Evidence from a randomized experiment. Santa Monica, CA: RAND Corporation.
10 Allowed charges refer to all charges under the physician fee schedule excluding hospital inpatient care, drug, laboratory, and emergency department visits (source:. http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianF…)
12 ACA Medicare PCIP: Practitioners (MDs and Non‐MDs) with primary care specialty designation meeting a threshold of 60 percent of primary care services*will receive 10 percent bonus on the Medicare paid amount from CY 2011 to CY 2016, $558 million in 2011 translates to an average of 2 percent increase in annual income for primary care physicians.
13 The Administration is proposing to extend this payment through Calendar Year 2015 and make it available to primary care nurse practitioners and physician assistants who practice independently. (add citation to 2015 Budget in Brief when it becomes available.)
The Lewin Group has reviewed the existing key health and labor economics literature for evidence regarding the potential impact of financial incentives on the supply of health care providers and services. The objectives of the literature review were to: (1) document the likely quantitative range of the effects of earnings increases (in the form of bonuses or other financial incentives) on the supply of primary care providers and services nationally or in underserved areas, and (2) explore the likely impact of the increase in Medicaid reimbursement rates for primary care providers on the volume of these providers and their services under Medicaid. This work can contribute to the broader understanding of provider behavior and the type and level of financial incentives that are likely to achieve the desired supply responses.
The literature that directly examines the Medicare bonuses and resultant impact on the supply of primary care providers and services is very limited. To address this limitation we expand our focus to include the labor economics literature. This broadened search then includes studies that address the behavioral impact of earnings on medical workforce. In what follows, we discuss the major findings from the existing literature on the effects of financial incentives (such as Medicare bonuses and increased Medicaid reimbursement rates) on primary care workforce and services. Overall, the scope of the literature review can be classified under the following categories:
There is considerable concern regarding a potential future primary care physician shortage and potential constriction of access to primary care. The availability of primary care is particularly important for public payer programs, such as Medicaid and Medicare. A recent Medicare Payment Advisory Committee (MedPAC) data book indicates that six percent of Medicare beneficiaries were looking for a new primary care physician in 2011. In addition, among those who tried to get an appointment with a new physician in 2011, 35 percent reported having difficulties. 14
It is worth noting that several studies (Bodenheimer et al, 2007; Vaughn et al, 2010) illustrated the large income gap between primary care providers and other specialties. Therefore, whether a very small increase in annual income, through the Medicare PCIP, would significantly influence provider behavior remains unclear. In addition, the time limited nature of the provisions may prove to be a major deterrent to a change in provider behavior. Any evidence around time‐limited bonus programs will likely show only a partial behavioral response from the targeted population. Lower bound take up rates should be expected in these programs because medical students and early career providers are unlikely to base career choices on temporary policy changes.
Historically, the Medicaid program has reimbursed physicians at a much lower rate than Medicare, paying just 66 percent of Medicare rates on average (Cunningham, 2011). Cunningham (2011) also documents that due to the low Medicaid reimbursement rates in several states fewer physicians accept Medicaid patients. In 2013 and 2014, ACA increases Medicaid reimbursement rates for certain services provided by primary care physicians to 100 percent of Medicare rates. Given the variability of Medicaid payments across states, this will be a substantial boost in payments for physicians in some states and less so in others. Current differential payment levels across states and any changes in payments over time can be exploited to examine the effect of raising Medicaid primary care reimbursement rates on the provision of primary care providers and services.
The discussion of the literature review is organized as follows: section A reviews the literature on the effect of earnings on the supply of primary care providers and services; section B discusses the evidence regarding the impact of financial incentives for primary care providers in underserved areas; section C examines the empirical evidence on the impact of state-specific changes in Medicaid reimbursement rates; and section D concludes with a summary of the major findings from the literature and their implications for understanding the allocative effects of bonus payments and other financial incentives.
14 MedPAC “ A Data Book: Health Care Spending and the Medicare Program,” June 2012, p. 97.
The ACA stipulates multiple programs with the aim of increasing the supply and utilization of primary care services. These programs all operate on the assumption that financial incentives, specifically directed toward increased earnings, are an effective way to promote an increase in primary care services and primary care providers. While these assumptions are based upon established economic theory, the evidence as to the programs’ effectiveness in practice is mixed.
While there is general consensus that expected earnings are a key driver of medical specialty choice (Bazzoli 1985; Nicholson and Propper 2011; Nicholson 2002; Vaughn et al. 2010), the evidence regarding the effectiveness of programs designed to attract medical students in certain specialties is inconclusive. Vaughn et al. (2010) argue that programs designed to affect the number of medical students choosing primary care have largely failed while others (Fournier & Henderson 2005; Lynch 1998; Ramsey 2001) argue that these programs have had a wide range of results that can be attributed to each programs’ individual composition.
The effect of earnings on labor supply in relation to the healthcare workforce is also a complex issue. There is wide consensus that increased earnings lead to an increase in the labor supply of health services providers (Askildsen and Baltagi 2002; Baltagi 2005; Rizzo and Blumenthal 1994), but the reported magnitude of this increase in labor supply varies widely. Values reported for the wage elasticity of the primary care labor supply range from 0.23 to 0.8. Furthermore, the effect of income on retirement decisions of physicians is not well understood.
Finally, the effect of earnings on the volume of primary care services is a related but distinct issue. Much like its counterparts, the effect of earnings on the volume of services is recognized to be significant and positive, but reported effects range widely: from a 10 percent reduction in Medicare fees leading to 1.8 percent to 6.6 percent reduction in the volume of office visits to 10 percent higher fees for primary care services raising the primary care E&M visits by 8.8 percent (Hadley et al. 2009; Reschovsky et al. 2012).
While the estimated effect of earnings on specialty choice is present and significant, the magnitude of this income effect and its relative importance as compared to other factors in deciding a specialty is contentious. Recent data from the residency match program in the US reveals that among 16,875 US Medical school senior applicants in 2012 about 35.5 percent were matched to primary care specialties such as internal medicine, family practice and pediatrics. 15 In 2010 the proportion matched to primary care (internal medicine, family practice and pediatrics) was 34.1 percent of 16,427 US Medical school senior applicants. 16 Between 1995 and 2006, the total number of physician residents in the US in primary care training programs increased by 6 percent, from 38,753 to 40,982 (Exhibit 1). Physician residents in specialty care increased by about 8 percent during the same period.
Exhibit 1. Number of Physicians in Residency Programs 17
| Type of Resident | Number of Resident Physicians | Percentage Change | |
|---|---|---|---|
| 1995 | 2006 | ||
| Primary Care Residents | 38,753 | 40,982 | 5.75 |
| Specialty Care Residents | 59,282 | 63,897 | 7.78 |
| All Physician Residents | 97,416 | 104,526 | 7.30 |
Nicholson and Propper (2011) argue that the rate of return to medical training and specialization is the key driver of choosing medical occupation and the choice of specialty within the area of medicine. The gap in median income between primary care physicians and specialists is well-publicized. For instance, using cross-sectional earnings data from 2008 Vaughn et al. (2010) report that the average primary care physician could expect to earn $2.5 million over his lifetime, net of income taxes, living expenses and education costs, versus $5.2 million for a cardiologist. Berenson et al. (2007) report that, according to the Medical Group Management Association (MGMA), between 2000 and 2004 median physician income for all primary care increased by 9.9 percent while average incomes of all non-primary care specialists increased by 15.8 percent. Arguably, given the income gap, raising the payment rate for primary care services relative to other services would impact the number of primary care physicians and raise the amount of primary care services they provide. Moreover, if the reimbursement rates vary by geographic region, this strategy can also affect the geographic distribution of services of primary care services.
In a related study, Bodenheimer (2007) attempts to explain this disparity in incomes. The author notes that the Resource-Based Relative Value Scale, which was initially designed to reduce the inequality between fees for office visits and for procedures, has failed to reduce the primary care–specialty income gap. He finds that this failure is due to four factors: (1) the volume of diagnostic and imaging procedures has increased more rapidly than the volume of office visits; (2) the process of updating the relative values units (RVUs) 18 associated with covered procedures is heavily influenced by the recommendations of the Relative Value Scale Update Committee (RUC), a majority of whose membership are specialists; (3) Medicare’s formula for controlling physician payments penalizes primary care physicians; and (4) private insurers tend to pay for procedures at higher rates than office visits relative to Medicare. They conclude that the program was designed with the correct motives but ultimately was weak and cannot achieve its purpose as currently formulated. Furthermore, incentives that favor specialists remain in the private market.
Nicholson (2002) also provides econometric evidence that the disparity in the expected earnings between primary care and other specialties has a significant influence on medical students’ decisions to choose primary care or another specialty. He observes that there is a persistent excess supply of residents to most specialties with relatively high lifetime earnings and a persistent excess demand for residents in primary care with relatively low lifetime earnings. His main contribution is to examine how differences in expected earnings affect the number of students who desire to enter a specialty rather than the number who actually enter the specialty. The study finds that the income elasticity ranges from 1.03 in family practice/pediatrics to 2.20 in radiology. 19 In other words, a 1 percent increase in the lifetime earnings of primary care providers, such as family practitioners, will increase the number of students ranking family practice as the most preferred choice by 1 percent which can be translated into an increase of equal magnitude in the supply of family practitioners.
However, there are studies that report comparatively less impact of expected earnings on the decision to choose primary care. Bazzoli (1985) found that medical students are more likely to choose primary care when the expected earnings are relatively large, but the effect is quite small. More specifically, a $10,000 (about 20 percent of the mean earnings in 1981) increase in the expected earnings in primary care relative to the non-primary care yields a 1.4 percentage point increase in the probability of choosing primary care.
Gagne and Leger (2005) have studied the specialty choice decision of Canadian physicians who practiced between 1989 and 1998. They find that a 9.1 percent reduction in relative fee-per-consultation for a general practitioner in Quebec and Saskatchewan, for example, would lead to a 0.4 percent reduction in the proportion of medical students entering general practice. The largest response is observed in Manitoba where the proportion of medical students entering general practice is estimated to decrease by 2.29 percent as a result of a 9.1 percent reduction in relative fee-per-consultation. The implied responsiveness of specialty choice to changes in earnings from this study and from other studies discussed in this section is summarized in Exhibit 2.
Vaughn et al. (2010) bolster this point by noting that programs designed to affect the number of medical students choosing primary care have largely failed because of the programs’ inability to affect relative incomes. By estimating career wealth accumulation across specialists, primary care physicians, physician assistants, business school graduates, and college graduates, the authors try to elucidate the true difference between payment of physicians and non-physicians, and between specialists and generalists within the physician group. They note that this result is to be expected as programs have done little and continue to do little to affect the disparity in expected lifetime earnings between primary care physicians and specialists. The authors also find that for a primary care physician’s lifetime earnings to equal those of a cardiologist the primary care physician would have to receive a bonus of $1.1 million upon completion of medical school.
Sivey and Scott (2012) use an econometric approach to address the question of the effect of lifetime earnings on training specialty choice based on a sample of Australian postgraduate doctors. Using a generalized multinomial logit model the authors find a statistically significant positive impact of earnings on the probability of choosing general practice training versus specialty training. Subsequently, they use the same model to simulate the effect of a $50,000 increase in annual earnings of general practitioners (GPs) on the probability of junior doctors choosing GP training. Specifically, the simulation result suggests that $50,000 additional earnings for GPs (a 27.8 percent increase over their current salary of $180,000) would lead to a 26.3 percent increase in the propensity of junior doctors to choose GP training. Therefore, the implied earnings elasticity of the propensity to choose GP training is 0.95, which is consistent with previous findings (Nicholson 2002).
Exhibit 2. Summary of Responsiveness of Specialty Choice to Changes in Earnings (Earnings Elasticity)
Note: earnings elasticity gives the percentage change in the outcome measure of interest (e.g., proportion of students ranking family practice or radiology as the 1 st choice) due to 1 percent change in earnings.
In an unpublished piece, Hogan and Bouchery (2010) estimate a multinomial logit model of the choices of internal medicine residents to remain in internal medicine and practice primary care, or to obtain a fellowship for further training in one of nine subspecialties of internal medicine and ultimately practice in that subspecialty. 20 The authors find that a 1 percent increase in earnings from one of the career paths, holding earnings in other specialties constant, increases entrants of male U.S medical graduates into that the examined specialty (Cardiology) by about 2.5 percent, but increases female entrants by about only 0.3 percent. They also find that increases in the length of additional training required for a subspecialty have a negative effect on the number of US medical graduates pursing that subspecialty and reduces the probability that US medical graduates pursue the specialty, but increases the probability that international medical school graduates pursue that subspecialty. 21
Expected lifetime earnings are not the only factor that influences decision making during specialty choice. Medical students assign a low level of prestige to a primary care career compared to other specialties. Students surveyed associate primary care with low income expectation, low class rank and high educational debt (Henderson, 1996). Students often enter medical school with a positive perception of primary care, but by the time they reach their fourth year they are increasingly likely to disagree with the assertions that primary practice is prestigious, adequately compensated, and allows more control over working hours (Lynch, 1998). It appears that students’ positive perceptions concerning primary care may change as they experience the more realistic professional demands on primary care physicians that can develop during medical school and as they observe their peers and role models, both within primary care and outside.
15 Source: NRMP Results and Data-2012 Main Residency Match (http://www.nrmp.org/data/resultsanddata2012.pdf)
16 US Medical school seniors who are matched into internal medicine can subspecialize, later on, in non-primary care specialty such as cardiology, endocrinology, oncology etc.
17 Steinwald B. Primary Care Professionals: Recent Supply Trends, Projections, and Valuation of Services. Statement in Testimony before the Senate Committee on Health, Education, Labor, and Pensions. Washington (DC): GAO; 2008. Available from: http://www.gao.gov/new.items/d08472t.pdf
18 RVU is a key component of the formula used under Medicare Physician Fee Schedule (PFS) to calculate payment rates for an individual service. There are three different RVUs: work RVU, practice expense (PE) RVU and malpractice (MP) RVU. Work RVU reflects the relative time and intensity associated with Medicare PFS service; PE RVU reflects the costs of maintaining a practice; and MP RVU reflects the cost of malpractice insurance. Source: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN…
19 Earlier studies of J.W. Hay (“Physicians’ specialty choice and specialty income”, Econometrics of Health Care, edited by G. Duru and J. Paelinck, Netherland Klwer Academic, 1991) and J. Hurley (“Physician choices of specialty, location and mode”, Journal of Human Resources, No. 26, 1991, pp. 47-71) did not account for uncertainty in entry to a specialty. However, they find that medical students are substantially responsive to expected income. These studies report income elasticities that range from 1 to 3.
20 Paul F. Hogan and Ellen Bouchery, “ A Model of Subspecialty Choice for Internal medicine Residents,” prepared by The Lewin Group for the American College of Cardiology. 2010.
21 After simulating the impact of decreasing cardiology training requirements from three years to two, the study finds that one-year decrease in training requirements would increase the percentage of male, U.S. medical school graduates choosing cardiology from 17.1 percent to 18.2 percent.
Consistent with the economic theory a large number of studies find evidence in support of a positive correlation between earnings and the labor supply of the health care workforce. This is in contrast to much earlier studies that relied only on aggregate time series data on physician services and fees to conclude that physician labor supply functions were backward-bending and physicians responded negatively to wage increases. 22 For instance, Steiger et al. (2010) observe that inflation-adjusted physician fees (weighted average of Medicare and private sector fees) decreased substantially between 1995 and 2005. The timing of the reduction in fees closely matched the observed decline in non-resident physician work hours. The study finds that the mean hours worked per week by physicians practicing in the US decreased by almost 7 percent between 1996 and 2008. Additionally, by 2006, physician fees were 25 percent lower than their inflation-adjusted 1995 levels. More recent studies, which use micro data to estimate traditional labor supply equation, generally find a small positive elasticity of physicians’ work hours with respect to wage increases. For instance, Rizzo and Blumenthal (1994) use the instrumental variable approach to estimate the unbiased effect of physician’s wage on the annual hours the physician spends on patient care. Their results based on all physicians suggest that a 10 percent increase in the wage rate yields a 2.7 percent increase in the physician’s annual work hours (i.e., wage elasticity of 0.27). When restricted to self-employed male physicians, they find a wage elasticity of 0.23. However, for female physicians they find a higher elasticity, with a 10 percent increase in the wage rate leading to a 4.9 percent increase in annual work hours. This work is generally supported by Baltagi et al. (2005) who find that a 10 percent wage increase would lead to a 3 percent increase in physician labor supply among hospital employed male physicians in Norway. Baltagi et al. (2005) note that the magnitude of the wage elasticity in this case may be relatively small because of hospital employed physicians’ tendency to earn a lower wage relative to self-employed physicians. 23
There are few studies that examine the effect of earnings on a physician’s decision to retire. Using micro data from Norway over the period of 1990-1992, Herneas et al. (2000) estimated a model to predict retirement behavior and simulated the effect of financial incentives on retirement decisions among those who were eligible to retire early (during 1990 - 1992) and who worked full-time in 1990. In their simulation, the annual pension from 1993 onwards is increased by 7.2 percent if the retirement eligible individuals continue to work full-time through 1992. This increase is equivalent to a 72.3 percent increase of the annual disposable pension. 24 The simulation result suggests that the average estimated probability of continuing to work full-time throughout 1992 will increase by almost 100 percent (from 38.4 percent to 70.6 percent) in response to the 72.34 percent hike in annual disposable pensions described above. 25 In other words, in the absence of any pension hike after 1993, only 38.4 percent of physicians working full time in 1990 would still work full time through 1992. However, if pension is raised by 72.3 percent from 1993 onwards for those who would continue to work full time through 1992, the simulation shows that 70.6 percent of physicians working full time in 1990 would still do so through 1992. They also estimated that the same financial incentives will lower the average estimated probability of partial retirement in 1992 (of retirement eligible workers) by about 54.7 percent (from 36.2 percent to 16.4 percent). Additionally, they find that other decisive factors influencing retirement decisions are the level of education, income, and marital status.
22 For an in-depth exposition of the empirical evidence and lack of support for a backward-bending physician labor supply, pleas e see Handbook of Health Economic, Vol 2, Chapter 14, Section 3.10
23 The nature of labor supply for Physicians and nurses differ greatly. There are some studies on the effect of wages on the labor supply of nurses. For example, Askildsen and Baltagi (2002) estimates a wage elasticity of nurses’ supply of labor between 0.7 and 0.8 depending upon the method of estimation. The authors argue that while theirs is a larger effect than other estimations have suggested it is still not a large effect relative to other professions. They also note that contract structure and type of work being performed significantly impact labor supply decisions and should not be ignored.
24 Wealth is defined as the discounted value of future annual disposable pensions and the increase in wealth is evaluated at the means of the data.
25 The expected remaining lifetime was then set at 18 years, which is close to the actual average for people in the relevant age groups in 1992.
The effect of earnings on the volume of primary care services is related to the previous questions but is a distinct issue that incorporates the ability of providers to impact the demand for services as a result of changes in their income. Dummit (2008) argues that, as the largest single payer, Medicare affects physician practice revenues directly through its payments and indirectly through its fee schedule, which many private payers use. Lower compensation for primary care physicians is one of the reasons that these specialties are less desirable. Reschovsky et al. (2012) report that over the past decade, Medicare fees and spending for specialist services (such as diagnostic tests and procedures) have gone up more rapidly than fees for E&M services, which primary care providers (PCPs) typically provide. Those higher payments have contributed to faster growth in specialist services than in E&M patient visits. Commercial insurers and state Medicaid plans often build their fee schedules on Medicare’s, further widening the income gap between PCPs and other physician specialists, and contributing to the shrinking number of medical students choosing to enter primary care. In this section we review how improvements in Medicare fees can influence the volume of health care services provided under Medicare.
Hadley et al. (2009) estimate the relationship between Medicare fees and the volume of eight specific services provided by physicians using data for 13,000 physicians from 2000-2001 and 2004-2005 Community Tracking Study Physicians Surveys. Since the fee schedule is one of the few policy tools that Medicare potentially has available to influence service volume, it is critical to have a better understanding of how changes in Medicare fees affect Medicare service volume. Their study finds that a 10 percent reduction in Medicare fees leads to 1.8 percent to 6.6 percent reduction in the volume of office visits (of various degrees of complexity). They argue that physicians may be more likely to respond to fee cuts by limiting their acceptance of new Medicare patients, rather than limiting visits by established patients.
Clemens and Gottlieb (2014) examine the changes in physicians’ reimbursement rates under Medicare before and after year 1997 when consolidation of geographic regions across which Medicare adjusts physician payments led to area specific price shocks. The study measures health care supply of all services using RVU. They find that health care supplied to Medicare patients (RVUs per patient) exhibits a relatively large long run elasticity of around 1.5 with respect to reimbursement rates. Their results are mostly driven by the stronger positive elasticity among elective procedures (e.g., eye and orthopedic procedures). When restricted to the analysis of the supply of E&M services their estimates lack precision and they find statistically insignificant short (1997-98) and long run (2001 to 2005) impact of the price shock on the supply of E&M services. However, the medium run (1999 and 2000) elasticity is precisely estimated to be 0.97 for E&M. They argue that the observed responses imply that the overall composition of services shifts toward more elective procedures as reimbursement rates increase. Finally, the number of patients and physicians per patient are almost unaffected by the change in the reimbursement rates.
Reschovsky et al. (2012) simulate the effect of a permanent 10 percent fee increase for primary care E&M services under Medicare. Their estimated primary care supply model suggests that higher primary care fees lead to increases in both the likelihood that PCPs will treat Medicare beneficiaries and, more importantly, the quantity of E&M services PCPs provide to Medicare patients. According to their analysis higher fees (10 percent increase permanently) for primary care beginning in 2011 raise the primary care E&M visits by 8.8 percent.
Thus, the likely range of changes in the volume of primary care visits in response to a long-term increase in Medicare primary care fees appears to be wide. Based on Hadley et al. (2009) and Reschovsky et al. (2012), a 10 percent increase in Medicare fees for primary care can potentially increase the volume of primary care visits in the range of 1.8 percent to 8.8 percent. However, due to the short-term nature of the Medicare PCIP (only 5 years) the observed impact of the incentive payment on the volume of E&M visits may be closer to the lower bound.
Access to health care in areas with insufficient health professionals has been an ongoing source of concern among policy makers. Expansion of health insurance coverage through the implementation of the ACA is likely to stimulate the demand for primary care in general, including underserved areas. Health Resources and Services Administration (HRSA) designates such areas HPSAs. These geographic areas meet a defined threshold of primary care physician to population ratio. Since 1987 Medicare has been paying bonuses to physicians providing primary care in rural HPSAs. In 1991 the bonus payment was increased from 5 to 10 percent and eligibility extended to services provided by physicians in urban HPSAs. Thus, this particular form of bonus payment has been in place for almost 25 years. Section 413(a) of the Medicare Modernization Act of 2003 put in place an additional 5 percent bonus payment for physicians practicing in Physician Scarcity Areas (PSAs). PSAs were those counties and rural zip codes in metropolitan statistical areas (MSAs) that represented the 20 percent of the Nation’s population with the lowest physician to population ratios. These areas often coincided with geographic HPSAs so that physicians practicing in those areas received a 15 percent additional bonus payment during 2005-2008 when the PSA bonuses were in effect (i.e., from January 2005 through June 2008).
In this section we review the literature related to the volume of these bonus programs and their potential effects on primary care services and providers. Programs to address this issue have historically been implemented with the assumption that financial incentives to practice in rural areas are effective in addressing the health professional shortage in given areas. This assumption is largely validated by the literature, with the effect of financial incentives shown to influence the distribution of physicians and health professionals. Importantly, the literature generally suggests a multifaceted approach to incentives, financial or otherwise. Many of the most successful programs evaluated below use recruitment of medical students with specific demographic markers to influence the distribution of physicians. Financial incentives have a broad range of reported specialty choice elasticities that range from 0.01 to 0.95. These discrepancies may also be somewhat determined by the type of financial incentive (e.g., grant, loan, postgraduate bonus).
In an early article on the HPSA bonus, Shugarman et al. (2001) estimate that, in 1991, the total amount of HPSA bonus was almost 31.6 million dollars. Their estimate shows that 58.3 percent of the total HPSA bonus payment went to the rural HPSAs; while the remaining 41.7 percent went to urban HPSAs. They also find that the total bonus payment grew to reach about 106 million dollars in 1996, but then gradually declined to almost 77 million dollars in 1998. The proportion of rural HPSA bonus decreased to 51.1 percent.
In a more recent study, Shugarman and Farley (2003) examined the trends in HPSA bonus payments for primary care specialties (family practice, general practice and internal medicine) under Medicare over the period of 1992-1998 using Medicare claims data for non-metropolitan area beneficiaries. They argue that the bonus payments largely targeted primary care. They find that in 1992 the payments for primary care services represented 29.7 percent of the total Medicare bonus payments for physician services to rural Medicare beneficiaries. The proportion gradually went up to 37 percent in 1998. Their analysis also showed that in 1992 payments for primary care services represented 14 percent of total basic Medicare payments for physician services and this share rose to 18.6 percent by 1998. However, 55.9 percent of all Medicare HPSA bonus payments for services to beneficiaries in non-metropolitan areas were made to primary care physicians. This proportion declined gradually to 49.7 percent in 1998. The authors claim that low levels of bonus payments in general, coupled with the documented declines in those amounts since 1994, may have undermined their future potential to support physicians practicing in rural areas. Their findings suggest that physicians were not claiming the extra payments that were available to them. Factors that could be contributing to such low uses of bonus payments include the extent to which physicians know about the payments, perceived value of the bonus to physicians, effects of administrative procedures on the ease of receiving them and concerns about the risk of audits. Nevertheless, their study highlights the role of bonuses in improving the payments and the supply of primary care services in HPSAs.
The literature regarding the effect of financial incentives in underserved areas on the choice of practice location of physicians is relatively scarce. Chou and Lo Sasso (2009) examined the impact of local characteristics on the practice location choices for newly trained physicians in New York between 1998 and 2003. Their empirical results suggest that PCPs without educational debt are attracted to HPSAs. In other words, they estimate that the propensity of choosing a location by a PCP is higher if the location is designated as an HPSA. However, the estimated propensity is lower if physicians have larger educational debt. Their study, however, addresses the effect of the HPSA status in general rather than any specific effect of the amount of HPSA bonuses.
In a review of rural incentive programs Sempowski et al. (2004) compare rural recruitment and retention programs in the United States against those in other countries (notably Canada and New Zealand). The authors look specifically at Return of Service (ROS) commitments wherein financial incentive is provided though assistance with medical school payment in return for a commitment to serve in a rural area. The authors note that programs offering financial incentives in exchange for ROS commitments to rural or underserviced areas have achieved their primary goal of short term recruitment. However, the authors note that in the US the lenient buyout opportunities have hindered the programs and limited their effectiveness. Sempowski et al. (2004) argue that the programs in Canada and New Zealand may have greater success with retention as compared to the US programs because the programs in Canada and New Zealand have a multi-faceted approach that includes the use of financial incentives along with prudent recruitment strategies.
Bolduc et al. (1996) provide a theoretical framework of physician’s choice of location. They develop a model to assess the effect of various incentive measures introduced in Quebec (Canada) on the geographical distribution of physicians across 18 regions during 1976-1988. The study specifically examines general practitioners’ choice of initial practice locations in Quebec. The utility of a particular alternative depends on, among other things, a measure of expected discounted value of lifetime earnings associated with this alternative. It is through changes in this variable that the impact of various income-based physician-location programs is simulated. Before 1982 there were substantial variations in the population to general practitioner (GP) ratio across different regions of Quebec. In order to redress geographic imbalances in the distribution of physicians the Quebec government introduced the Differential Remuneration Program (DRP) in 1982 that raised the fees (relative to the base fees to general practitioners in underserved regions compared to the regions with relatively lower population to GP ratios. Among other incentive measures, annual study grants of $10,000 have been offered (since 1982), tied to a commitment to work in these underserved regions during a number of years equal to the number of grants received. A settlement grant program has also been available, since 1984, for physicians who choose to practice in these regions. This program provides an annual allowance for a maximum of 4 years. It varies from $5,000 to $10,000 (nontaxable) for a physician paid by unit of service, depending on the shortage of physicians in the locality. Whereas the differential remuneration program influences location choices through differential pricing of physicians’ services by location, the grant program affects location choices through a lump sum increase in income for a short duration (4 years).
Bolduc et al. (1996) find that on average, a 10 percent increase in the general practitioner fees for medical services in a region increases the propensity of a beginning GP to work in this region by 7 percent. Thus the implied elasticity of location choice probability with respect to fee increases is about 0.7. However, this elasticity varies across regions: it is higher in remote regions (with a maximum of 1.28). On the other hand, on average, the elasticity of location choice probability with respect to non-labor incomes, such as study grants, is estimated to be about 1.11. In other words, a 10 percent increase in the study grants tied to a commitment to work in the underserved regions, leads to an 11.1 percent increase in the probability of GPs choosing these underserved regions as their starting practice location. However, their findings largely depict redistribution of GPs across regions within Quebec rather than showing any increase in the total number of GPs in Quebec.
Despite differences in the institutional framework between the US and Canada, the findings from Bolduc et al. (1996) provide some valuable insights into the potential effects of financial incentives that vary across locations. The remaining important issue is to identify how bonus payments affect the annual earnings of physicians in HPSAs. Only then, based on findings from the literature, can one assess the potential impact of the earnings shock in HPSAs on primary care physicians’ choice of practice location. Holmes (2005) addresses this question directly. Using a database containing the location of physicians at 5-year intervals the author compares the locations chosen by alumni and non-alumni of programs within the United States charged with increasing physician supply in underserved areas. This analysis provides insight into the types of students that choose to enroll in programs such as the National Health Service Corps (NHSC). The author notes that participation in this program consists disproportionately of minorities from private, expensive schools. This suggests that scholarships (and hence the lack of debt burden) may be an influential factor in participation in the NHSC. The multinomial logit model employed by Holmes (2005) shows that students which graduate from an institution with a focus on primary care are also more likely to enroll in the NHSC. Using this model, Holmes (2005) concludes that the elimination of the NHSC program would lead to a 10-11 percent decrease in the supply of recent graduates in underserved communities.
Rabinowitz et al. (2001) examine the history and results of The Physician Shortage Area Program (PSAP) of Jefferson Medical College (Philadelphia, PA). The PSAP is intended to address the shortage of primary care physicians in rural Pennsylvania. The authors’ analysis uses a cross section of Jefferson Medical College Graduates from 1978 to 1993 to determine which characteristics are predictive of becoming a rural primary care physician (PCP). Of the characteristic variables collected in the data, freshman year plans for family practice, being in PSAP, having a NHSC scholarship, male sex, and taking elective senior family practice rural preceptorship were independently predictive of primary care in a rural area. However, among non-PSAP graduates with two key selection characteristics of PSAP students (having grown up in a rural area and freshman year plans for family practice) were 78 percent as likely as PSAP graduates to be a rural primary care physician, and 75 percent to remain rural PCPs. The authors note that this result suggests the most influential area of the program is the admissions component, not the financial component. Supporting evidence for this conclusion is provided by Brooks (2002) who found that rural upbringing and specialty preference were most strongly correlated with recruitment of physicians to rural areas. Growing up in a rural area along with the student’s expressed plan to become a primary care physician were associated with a 36 percent likelihood of a graduate practicing in a rural area compared with 7 percent for individuals without these preferences.
Although most studies found that there was no correlation with age, gender, race, or marital status (Horner, 1993; Looney, 1998; Rabinowitz, 1999) a few studies determined that men have a greater likelihood of rural practice than women (Fryer, 1997; West, 1996). However, women PSAP graduates were more than twice as likely as non-PSAP women to practice in rural areas (31.7 percent versus 12.3 percent) (Rabinowitz, 2011). Importantly, none of these articles list financial incentives as an important factor in recruitment and retention of primary care physicians in rural areas.
The availability of primary care is particularly important for public payer programs, such as Medicaid and Medicare. Historically, Medicaid has been the lowest payer for primary care services relative to Medicare, paying just 66 percent of Medicare rates on average. 26 Cunningham et al. (2009) report that fewer physicians accept new Medicaid patients in response to the low Medicaid reimbursement rates in several states. Zuckerman et al. (2009) describe that in 2008 average primary care physician fees under Medicaid ranged from 57 percent of the national average in Rhode Island to 226 percent of national average in Alaska. They also find that after a strong Medicaid fee growth during 1998-2003, Medicaid fees fell relative to inflation during 2003-2008. Despite the slowdown in overall fee growth, Medicaid fees for primary care services kept pace with inflation. ACA increases Medicaid reimbursement rates for certain services provided by primary care physicians to 100 percent of Medicare rates in 2013 and 2014. Given the variability of Medicaid payments across states, this could be a substantial boost in payments for physicians in some states and less so in others.
The findings in this section focus on the comprehensive effect of a relative rate increase, both on services provided and patient’s utilization of those services. While evidence is mixed, the literature indicates significant effects of increased Medicare reimbursement on both the provision and utilization of primary care services. Reported elasticities range between 0.41 in national estimates to -0.06 in some state level analyses. This broad range suggests varying evidence and a need for greater examination given the importance of this question.
26 Small, D.M. and T. McGinnis, (2012): “Leveraging the Medicaid Primary Care Rate Increase: The Role of Performance Measurement”: Center for Health Care Strategies, Inc.
Systemic Medicaid changes have the potential to alter the primary care environment across all states. Cunningham (2011) considers a regression-based approach to identify the causal effect of increases in Medicaid reimbursement rates relative to the Medicare rate on the propensity of primary care physicians accepting new Medicaid patients. He reported, prior to the 2012 Supreme Court decision (National Federation of Independent Business et al. vs Sebelius et al. 27 ), that once the ACA is implemented Medicaid eligibility will expand to cover as many as 16 million more poor and low-income adults by 2019 (an increase of more than 25 percent). To meet the resultant surge in demand for primary care services, ACA provides financial incentives to encourage higher participation of primary care physicians in Medicaid. Specifically, the ACA raises the Medicaid reimbursement rates for certain services provided by primary care physicians up to 100 percent of Medicare rates in 2013 and 2014. This study uses primary care physicians from the HSC 2008 Health Tracking Physician Survey and exploits the existing state level variation in Medicaid reimbursement rates (as a percentage of the Medicare rate). The author groups the states in three categories (low, medium and high) based on PCPs to population ratios.
This study shows that in 2008 the average Medicaid reimbursement rate for low-PCP states was about 81.6 percent of the Medicare rate; while for medium and high-PCP states the average rates were 64.3 percent and 54.8 percent, respectively. The national average of the Medicaid reimbursement rate was 66.2 percent of the Medicare rate. Cunningham (2011) examines the effects of Medicaid reimbursement rates on PCP acceptance of Medicaid patients, while accounting for differences in physician practice, patient and health care market characteristics. The results show that higher Medicaid reimbursement rates are associated with a greater probability of PCPs accepting all or most new Medicaid patients, although the effects are relatively modest. For PCPs, a 10-percentage point increase in the Medicaid/Medicare fee ratio for primary care is associated with only a 2.1-percentage-point increase in PCP Medicaid patient acceptance. The study reports that the national average Medicaid reimbursement rate relative Medicare in 2008 was at 66.2 percent and the national average acceptance rate of new Medicaid patients by PCPs was 41.5 percent. Therefore, the implied elasticity of accepting primary care patients with respect to the payment rate is about 0.33. 28 In other words, if the Medicaid fee relative to the Medicare rate goes up by 10 percent then the acceptance of new Medicaid patients by PCPs goes up by 3.3 percent. Excluding pediatricians, the effect of reimbursement on Medicaid acceptance is slightly higher: the implied elasticity of accepting primary care patients with respect to the payment rate is about 0.41. In the context of the parity in Medicaid and Medicare reimbursement rate under the ACA, empirical findings by Cunningham (2011) can serve as a benchmark for the likely positive effect of higher Medicaid reimbursement rates on the access to primary care services.
Other studies bolster this finding. Shen and Zuckerman (2005) study the effects of Medicaid payment generosity on access and care for adult and child Medicaid beneficiaries. The authors use data comparing the experiences of Medicaid beneficiaries with groups that should not be affected by Medicaid payment policies (the uninsured) using a difference-in-differences model. Shen and Zuckerman (2005) find that higher payments do increase the probability of having a usual source of care and the probability of having at least one visit to a doctor or other health professional. Specifically, they find that a one unit increase (equivalent to a 10 percent increase) in the payment generosity index 29 leads to a 1.5 percentage point increase in the probability of having a usual source of care and a 1.6 percentage point increase in having at least one visit to a health professional. 30 Importantly, payment generosity was noted to have no effect on the probability of receiving preventive care or the probability of having unmet needs. The authors argue that this weak association between increased payments and utilization of services is due to the higher correlation between payment increases and participation by physicians, with a secondary effect on utilization.
27 U.S. Supreme Court’s decision in the case challenging the constitutionality of the Affordable Care Act (ACA: http://www.supremecourt.gov/opinions/11pdf/11-393c3a2.pdf
28 Implied Elasticity is (2.1/41.5)/(10/66.2) or 0.33. After excluding Pediatricians the acceptance rate of Medicaid patients among PCPs is about 38.5 percent and a 10-percentage point increase in the Medicaid/Medicare fee ratio for primary care is associated with only a 2.4-percentage-point increase in PCP Medicaid patient acceptance. Therefore, the implied elasticity is (2.4/38.5)/(10/66.2) or 0.41.
29 The Medicare payment generosity index is defined as the Medicare capitation rate in a county divided by the median Medicare capitation rate in the nation in a given year. Average is defined to be 10.
30 These can be interpreted as elasticities. Implied elasticity would be 0.15 and 0.16 respectively.
To better understand the mechanism by which systemic changes in the Medicaid system will be implemented and the broad range of environments affected it is informative to review Medicaid changes at the state level. Zuckerman et al. (2004) illustrate that Medicaid physician fees increased, on average, by 27.4 percent between 1998 and 2003, with primary care fees growing the most. On average, the cumulative percentage change in the Medicaid primary care fee was about 41.2 percent between 1998 and 2003. The authors note that there was considerable variation in primary care fees across states. Seven states (District of Columbia, Georgia, Indiana, Kentucky, Maine, Rhode Island, and South Dakota) left primary care fees almost unchanged, while two states (Iowa and New York) raised them by more than 100 percent. States with the lowest relative fees in 1998 increased their fees the most, but almost no states changed their position relative to other states or Medicare, since Medicare rates also increased over the period. Subsequently, the study finds that primary care physicians’ acceptance of Medicaid patients in high-fee states was about 18 percentage points higher than the low-fee states (61 percent versus 43 percent) in 1997; while in 2001 the gap is reduced to 11 percentage points (58 percent versus 47 percent). The national average of primary care physicians’ acceptance of most or all new Medicaid patients was 53 percent in 1997 and 54 percent in 2001. Moreover, large fee increases (e.g., low-fee states experienced the largest fee change on average) were associated with primary care physicians’ greater willingness to accept new Medicaid patients: the rate of primary care physicians’ acceptance of new Medicaid patients in these low-fee states went up from 43 percent in 1997 to 47 percent in 2001. Although their study shows some evidence that a Medicaid fee increase is associated with increased Medicaid participation among primary care physicians, it does not provide a direct link between Medicaid reimbursement rates relative to Medicare and physicians’ acceptance of Medicaid patients.
Bindman et al. (2003) examine California in particular and focus on the relationship between Medicaid fee increases and the prevalence of managed care in the Medi-Cal system. The authors note that in August of 2000 a fee increase raised physician Medicaid reimbursement from an average of 57.7 percent to 65.2 percent of the average Medicare payment in California. This amounts to a fee increase for a typical office visit from approximately $18 to $24. The study used cross-sectional surveys in 1996 and 2001 on both primary care physicians and specialists. Controlling for physician demographics and specialties the authors found no increase in Medi-Cal participation. Their study notes that between 1996 and 2001, despite payment increases, the number of Medi-Cal primary care physician equivalents dropped from 57 to 46 per 100,000 patients. 31
Mukamel et al. (2012) address the effect of similar financial incentives in California’s Medicaid system but from the standpoint of nurse staffing levels. Using separate models for three staffing types, RNs, LPNs, and CNAs, the authors determined that financial incentives were only a significant factor in increasing hours per resident day (hprd) for RNs. They note that expected nursing home reimbursement rate increases in 2008 were associated with increased RN staffing levels in 2006. They estimate the effect at around a 2-minute increase (0.035 hrpd) for each $10 increase in payment rate. This amounts to a 10 percent increase in staffing over 2005 base levels. The authors explain that this relatively small increase in staffing might be partially explained by the financial incentives original intent that is, to influence labor expenditures and not directly influence staffing levels. The authors note there may have been a change in wages and benefits for all three groups, but that it was not measured in this study.
Finally, Coburn et al. (1999) examined the effect of Medicaid fee changes on physician participation and enrollee access in Maine and Michigan using multiple natural experiments. The authors found that changes in Medicaid fees observed in either state over any observed period had no substantial impact on either physician participation or enrollee access and utilization. 32 In one case in Maine, after an increase of 47.5 percent in Medicaid reimbursement rates, primary care physician participation fell by 1 percent (from 477 to 471). 33 After a second increase of 24.5 percent, participation increased by only 2 percent. 34 This result is mirrored in Michigan where participation increased by only 2 percent after a reimbursement increase of 7.9 percent and decreased by 0.6 percent after a cut of 16.6 percent and fell again by 0.2 percent after a restoration of 19.6 percent. The authors note that these small changes in physician participation hold even when adjusting for lagged responses in both cases. The authors found similar results when examining the utilization of services. Using ambulatory care as a proxy for utilization of services in general, the authors found that changes in the proportion of beneficiaries with at least one visit in a month and in the average number of visits by beneficiaries with at least one visit are not in a direction consistent with the fee changes and are all very small in magnitude. The authors note that these results also do not change when estimated in the long run. However, a major confounding factor in these results, as the authors note, is the relative size of Medicaid payment rate increases compared to those of the private sector fees. The authors state that most gains relative to the private market were quickly eroded.
31 A physician equivalent is defined as one full time physician providing full time working hours per week (40 hrs) in a given specialty. For example, a physician who provides 20 hours of Family Medicine is counted as 0.5 of a physician equivalent in Family Medicine.
32 The study has given due consideration to the changes in Medicaid payment relative to the payments by other payers. The authors use the ratio of Medicaid payments to charges as an index of changes in relative payments. They have also confirmed with Blue Cross Blue Shield (BCBS) of Michigan (which serves 49 percent of the state’s health insurance market) that BCBS’s payments-to-charge ratio for all physician services did not change substantially.
33 The corresponding relative fee change (i.e., Medicare relative to charges) is 40.2 percent.
34 The corresponding relative fee change (i.e., Medicare relative to charges) is 25.8 percent.
In order to inform our empirical estimation, the Lewin Group has explored the health and labor economics literature to understand the nature and the size of the impact of any financial incentives on the labor supply behavior of PCPs and the resultant impact on the availability of primary care services. The main objective of this review is to document the prior empirical evidence of the impact of financial incentives on raising the supply of primary care workforce, the volume of services, impact on medical graduates’ propensity to participate in primary care, PCPs’ retirement decision, etc. This review also evaluates the past evidence on the effect of bonuses shortage areas and their effectiveness in redistributing and retaining primary care workforce. Finally, the review of the literature also focuses on the state-specific experiences with changes in their respective Medicaid payment rates for primary care and the resultant impact on the supply of PCPs, their rate of acceptance of Medicaid patients and the volume of primary care services such as office visits or visits for E&M services.
Affecting the choice of specialty by a medical student is one way by which the supply of primary care services may be increased. Several studies (e.g., Nicholson, 2002; Sivey and Scott, 2012) find that the propensity of medical graduates choosing primary care as their specialty would go up by 9.5-10 percent in response to a 10 percent increase in their earnings (i.e., earnings elasticity of 0.95-1.0). Thus even if bonus payments have the potential to influence the inflow of medical students into primary care, the magnitude of that impact would depend largely on the size of actual bonus payments relative to PCPs’ earnings and how long such payments are in place. These two factors will determine the contribution of the Medicare bonus to the life-time earnings of primary care providers.
Another way to affect the supply of primary care services is to provide financial incentives for existing providers with the aim of increasing their labor supply. Past research (e.g., Rizzo and Blumenthal, 1994; Baltagi et al., 2005) estimates that a 10 percent increase in wage earnings would yield a 2.3 ̶3 percent increase in their annual work hours. This low wage elasticity suggests that influencing the supply of primary care labor with direct fee increases alone is likely to be costly. The increased fee payments will also likely have an effect on the volume of primary care services. However, compared to the wage elasticity, the change in volume of services in response to fee increases is relatively low. Empirical evidence from the literature (e.g., Hadley et al., 2009; Reschovsky et al., 2012) suggests that a 10 percent change in Medicare fees would change the volume of office visits or E&M related visits by 1.8 to 8.8 percent in the same direction.
The numerical estimates of the effect of financial incentives in underserved areas on the choice of practice location of physicians in the US are relatively scarce. An important study based on Canadian data finds that on average, a 10 percent increase in the general practitioner (GP) fees for medical services in a region increases the propensity of a beginning GP to work in this region by 7 percent (Bolduc et al., 1996). Thus the implied elasticity of location choice probability with respect to fee increases is about 0.7. Several studies highlight the role of bonuses in improving the payments and the supply of primary care services in HPSAs in the US. However, estimating the true contribution of bonuses in underserved areas in boosting physicians’ earnings would require additional research.
Past research on state-specific increases in Medicaid and their resultant impact is relatively sparse. However, several studies find a positive correlation between the Medicaid reimbursement rate and acceptance rate of Medicaid patients among PCPs. Cunningham (2011) finds that the effect of increase in Medicaid reimbursement rate on the propensity of accepting primary care patients is positive but small in magnitude. Coburn et al. (1999) finds positive impact of Medicaid fee changes on physician participation and enrollee access in Maine and Michigan; while Bindman et al. (2003) did not find significant effect of Medicaid fee increase on the participation rate of primary care physicians in California.
Despite several empirical results regarding the potential magnitude of the effect of different financial incentives, the estimated effect of Medicare bonuses or improvement in Medicaid reimbursement rates under ACA may not be substantial. This is primarily due to the size and the temporary nature of these positive earnings shocks. The empirical evidence on the effect of this type of short-term pay increase is almost non-existent in the literature. However, the ranges of the effects of long-term earnings shocks from our review of the literature can inform policy makers about the likely magnitude of the impacts of these income-augmenting policies for PCPs if they are sustained for a longer duration.
The Medicare primary care incentive is available to eligible primary care practitioners for services provided under selected categories of E&M. An eligible primary care practitioner is a physician, nurse practitioner, clinical nurse specialist or a physician assistant who satisfies the following criteria:
This temporary payment is available for primary care services furnished by an eligible primary care practitioner on or after January 1, 2011 and before January 1, 2016. The payment is made on a quarterly basis and it amounts to 10 percent of the payment amount for the Part B-covered primary care services furnished by the eligible provider.
Based on data regarding all the Medicare PCIP recipients in 2011 and 2012 we observe that in 2011 there were 162,342 providers that received the PCIP, with the majority of physicians specialized in family medicine and internal medicine (Exhibit 3). Also, nurse practitioners account for more than half of non-physician recipients in both 2011 and 2012. Finally, there was an increase in the number of physician PCIP recipients across all eligible specialties in the second year the payment was in effect. The number of all eligible types of non-physician PCIP recipients also increased. These estimates are consistent with the statistics reported by CMS 35 .
Exhibit 3: Number of PCIP Recipients under Medicare by Specialty, 2011-2012
| Specialty | Year 2011 | Year 2012 |
|---|---|---|
| Total | 162,342 | 185,312 |
| Physicians | 121,140 | 133,880 |
| Internal Medicine | 54,062 | 62,554 |
| Family Medicine | 63,227 | 66,560 |
| Pediatrics | 2,711 | 3,426 |
| Geriatrics | 1,140 | 1,340 |
| Non-Physicians | 41,202 | 51,432 |
| Clinical Nurse Specialist | 466 | , |
| Nurse Practitioner | 27,698 | 33,940 |
| Physician Assistant | 13,038 | 16,899 |
Note: Actual PCIP recipients; eligibility based on conditions 2 years prior to the PCIP payment year.
The specific PCIP-eligible services and their corresponding Current Procedural Terminology (CPT) codes are as follows: (1) office and other outpatient visits (99201 through 99215); (2) nursing facility, domiciliary, rest home, or custodial care (99304 through 99340); and (3) home services (99341 through 99350).
Medicare claims data include the Healthcare Common Procedure Coding System (HCPCS) corresponding to each claim submitted by providers. Since level I of HCPCS codes is comprised of CPT codes, HCPCS codes associated with claims can be used to determine bonus-eligible E&M services.
The key questions that we examined using the Medicare data include:
To explore these topics, we used a customized data set constructed at the provider level. This data set includes all the claims submitted by the entire universe of Medicare providers in each year from 2005 to 2011. The content of this customized data set is similar to the Limited Data Set (LDS) version of the Medicare Carrier File (which is also known as the Physician/Supplier Part B Claims) available from CMS Research Data Assistance Center (RESDAC). Subsequently, in the discussion that follows we will refer to the customized claims level data set for all Medicare providers as the Provider Carrier File (PCF). Most of the claims in our PCF are from non-institutional providers, such as physicians, physician assistants, clinical social workers, and nurse practitioners. Key variables in this file include:
Provider specialty, place of service, and geographic location (such as zip code)
We constructed a provider level pooled data set (PPD) from the claims level data in the PCF over the period 2005-2011. This pooled data set includes information such as provider specialty, volume of primary care services (based on HCPCS codes), volume of PCIP eligible services, distribution of providers by volume of services, their annual Medicare allowed charges, their geographic location, and other related information, over a longer time horizon. In addition, the original PCF included a National Provider Identifier (NPI) for each provider. Subsequently, each provider was linked by NPI to Provider360 data (available from Lewin Group’s parent company Optum Inc.) and the AMA Physician Master File to add provider characteristics such as provider demographics (e.g., age, gender), provider designation, medical school, practice group information, specialty and practice location. We also added geographic location specific characteristics by linking the provider level data with the Area Resource File (ARF) based on the practice location information of providers. The ARF data are maintained by the Health Resources and Services Administration (HRSA). The main advantage of this pooled data set is the ability to track providers over time and capture changes in their volume of services in response to Medicare payment incentives using a pre-and-post analysis design.
We were interested in estimating the impact of the PCIP on the supply of PCPs and patients’ access to their services. We measured improvements in access to care by studying changes in the volume of primary care services provided and the number of PCP providers. Both the supply of PCPs and volume of services are measures of access to care previously used in the literature. 36 In addition, we investigated the impact of the PCIP on the allowed charges associated with eligible E&M claims.
First, we examined the trend in the number of eligible providers submitting Medicare claims. An increase in the number of primary care providers relative to the population is expected to improve access to primary care. As shown in Exhibit 4, the number of PCPs accepting Medicare patients increased steadily over the study period with an approximate 40 percent increase in the number of providers treating Medicare patients from 2005 to 2011. This trend is common to all four physician specialties under study. 37 In addition, the number of non-physician practitioners more than doubled over this period. This significant increase in the number of non-physician providers, especially nurse practitioners, has been documented elsewhere. 38
Exhibit 4: Number of Primary Care Providers under Medicare by Specialty, 2005-2011
| Specialty | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 |
|---|---|---|---|---|---|---|---|
| Total | 184,990 | 201,594 | 233,447 | 253,059 | 267,353 | 282,859 | 301,283 |
| Physicians | 138,356 | 147,771 | 165,150 | 173,018 | 178,784 | 185,070 | 191,930 |
| Internal Medicine | 69,391 | 74,411 | 83,117 | 87,090 | 90,291 | 93,904 | 97,526 |
| Family Medicine | 61,438 | 65,205 | 72,247 | 75,132 | 77,536 | 79,891 | 82,298 |
| Pediatrics | 6,539 | 7,045 | 8,527 | 9,447 | 9,543 | 9,757 | 10,555 |
| Geriatrics | 988 | 1,110 | 1,259 | 1,349 | 1,414 | 1,518 | 1,551 |
| Non-Physicians | 46,634 | 53,823 | 68,297 | 80,041 | 88,569 | 97,789 | 109,353 |
| Clinical Nurse Specialist | 1,784 | 1,934 | 2,188 | 2,304 | 2,370 | 2,446 | 2,508 |
| Nurse Practitioner | 23,610 | 27,450 | 35,286 | 42,144 | 46,973 | 52,472 | 59,505 |
| Physician Assistant | 21,240 | 24,439 | 30,823 | 35,593 | 39,226 | 42,871 | 47,340 |
Our second measure of supply of primary care services is the volume of claims submitted by primary care providers for E&M services. As presented in Exhibit 5, the volume of E&M claims submitted by physicians increased by roughly 9 percent between 2005 and 2008. E&M claims took a slight dip in 2009, increased in 2010, and then stabilized in 2011 at roughly the levels in 2008. The same general increasing trend applied to each of the four eligible physician specialties, with the exception of geriatrics, which experienced a constant and substantial increase in E&M claims of 52 percent over the study period. Internal medicine physicians provided the majority of services, generating more than 50 percent of E&M claims each year over the study period. Family physicians are the second largest group of providers to supply E&M services, representing about 40 percent of the total, followed by geriatricians and pediatricians.
Consistent with the increase in the number of non-physicians documented above, we observe an even more dramatic increase in the total number of E&M claims submitted by non-physicians (clinical nurses, nurse practitioners and physician assistants). The volume of E&M claims more than doubled over the study period, from roughly 9 million in 2005 to more than 20 million in 2011.
Exhibit 5: Total Number of PCIP Eligible E&M Claims submitted by All PCPs under Medicare by PCP Specialty, 2005-2011
| Specialty | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 |
|---|---|---|---|---|---|---|---|
| Physicians | 105,943,390 | 107,978,615 | 111,700,420 | 115,408,741 | 114,881,401 | 117,265,160 | 115,329,828 |
| Internal Medicine | 60,279,101 | 61,222,893 | 63,082,429 | 64,946,744 | 64,244,760 | 65,447,440 | 63,698,392 |
| Family Medicine | 44,352,228 | 45,264,171 | 47,011,232 | 48,776,874 | 48,891,712 | 49,977,085 | 49,767,310 |
| Pediatrics | 334,997 | 352,594 | 360,508 | 365,170 | 387,636 | 391,312 | 377,604 |
| Geriatrics | 977,064 | 1,138,957 | 1,246,251 | 1,319,953 | 1,357,293 | 1,449,323 | 1,486,522 |
| Non-Phys. | 8,885,528 | 10,366,281 | 11,979,963 | 13,710,969 | 15,376,840 | 18,008,471 | 20,477,006 |
| Clinical Nurse Specialist | 6,083,315 | 7,068,153 | 8,117,610 | 9,212,329 | 10,298,679 | 11,987,059 | 13,561,380 |
| Nurse Practitioner | 153,463 | 165,033 | 168,030 | 200,074 | 228,899 | 260,618 | 296,206 |
| Physician Assistant | 2,648,750 | 3,133,095 | 3,694,323 | 4,298,566 | 4,849,262 | 5,760,794 | 6,619,420 |
With both the aggregate number of E&M claims and the number of providers rising over time, we further explore the change in the volume of claims per provider over time. In other words, we examined whether the increase in the aggregate number of claims could be due to the increase in claims per provider or whether it is just due to the increase in the number of providers.
Inspection of Exhibit 6 reveals that in the case of all physicians the average number of eligible E&M claims per provider in 2011, was lower than in 2005. For instance, the average number of eligible E&M claims for internal medicine was 653 in 2011 compared to the higher value of 869 in 2005. The decreasing trend in average claims per physicians may be due to the increase in the number of PCPs in the absence of a substantial increase in the patient population.
Exhibit 6: Average Number of PCIP Eligible E&M Claims per PCP
under Medicare by Specialty, 2005-2011
Finally, in the case of non-physicians, there was an overall increase in the average number of E&M claims submitted by physician assistants (PA), nurse practitioners (NP) and clinical nurse specialists (CNS) after 2009 (see Exhibit B2, Appendix B). For example, the number of claims per PA increased from 125 in 2005 to almost 140 in 2011. On the other hand, the number of claims per NP was 253 in 2005, then declined to 219 in 2009 and then increased to about 228 in 2011. The increase in the average number of claims submitted suggests that the dramatic increase in services provided is due to both an increase in the number of providers and in the number of services provided by each non-physician. The average number of claims per PCIP recipients by specialty and the average allowed charges per PCIP recipients by specialty are presented in Appendix B Exhibit 12 and 13 respectively.
So far, we have focused on the level of E&M services provided, measured in terms of number of claims and the number of providers. Next, we turn to the dollar value associated with E&M claims measured using allowed charges. As shown in Exhibit 7, the total allowed charges (in million dollars) for eligible E&M claims increased for all providers over the period of analysis. Overall, total allowed charges increased by 58 percent, with internal medicine and family medicine physicians accounting for most of this increase. It is also noteworthy that the value of claims submitted by non-physicians increased substantially over the same period, by a factor between 2 and 3.
Exhibit 7: Total Allowed Charges (in million $) for the PCIP Eligible E&M Claims submitted by All PCPs under Medicare, 2005-2011
| Specialty | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 |
|---|---|---|---|---|---|---|---|
| Total | $6,687 | $7,091 | $7,960 | $8,556 | $8,990 | $10,193 | $10,589 |
| Physicians | $6,271 | $6,575 | $7,343 | $7,813 | $8,119 | $9,079 | $9,274 |
| Internal Medicine | $3,671 | $3,830 | $4,251 | $4,506 | $4,644 | $5,182 | $5,231 |
| Family Medicine | $2,520 | $2,645 | $2,982 | $3,183 | $3,340 | $3,742 | $3,881 |
| Pediatrics | $20 | $21 | $23 | $24 | $26 | $30 | $30 |
| Geriatrics | $61 | $78 | $87 | $100 | $108 | $125 | $131 |
| Non-Physicians | $416 | $517 | $617 | $743 | $871 | $1,114 | $1,316 |
| Clinical Nurse Specialist | $287 | $358 | $421 | $507 | $592 | $749 | $878 |
| Nurse Practitioner | $8 | $9 | $9 | $11 | $14 | $17 | $20 |
| Physician Assistant | $122 | $150 | $187 | $225 | $265 | $349 | $418 |
As shown in Exhibit 8, the average allowed charge per PCP for E&M claims increased slightly for internal medicine physicians and pediatricians after 2009 (also see Appendix B Exhibit B2). The average value of E&M claims increased for the other PCPs, but not as fast as the total value of these claims. Given the moderate increase in the average allowed charges for E&M claims, the substantial increase in the aggregate allowed charges is likely due to the increase in the number of claims, which in turn, as discussed above may be driven by the increase in the number of providers. Another important observation is that although the average number of claims submitted by physicians declined over the 2005-2011 period, the average allowed charges remained the same or even increased. This observed increase in allowed charges per provider, despite the documented decline in the number of claims, may reflect changes in the composition of services that physicians are providing. We hypothesize that this change in the composition is due to an increase in the supply of services that take more time and which are typically associated with higher charges. We explore this hypothesis in the following section.
Exhibit 8: Average Allowed Charges ($) for the PCIP Eligible E&M Claims per PCP under Medicare by Specialty, 2005-2011
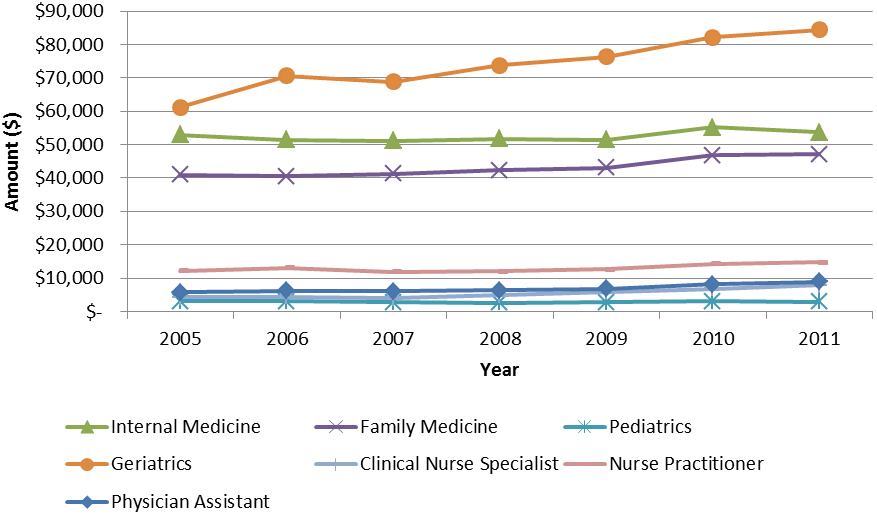
Finally, we constructed the proportion of practitioner’s allowed charges under the Medicare fee schedule (excluding hospital inpatient admission and emergency room visits) that are for PCIP eligible primary care services. As observed in Exhibit 9, for both physicians and non-physicians, the proportion of services that are PCIP eligible varies across specialties and is in general steadily increasing over the observation period. However, compared to primary care physicians, the non-physicians experienced a much larger percentage change in the share of allowed charges that are associated with PCIP eligible services.
Exhibit 9: Share of Allowed Charges for PCIP Eligible E&M Claims by Specialty,2005-2011
| Specialty | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 |
|---|---|---|---|---|---|---|---|
| Physicians | |||||||
| Internal Medicine | 58.3% | 59.0% | 61.1% | 60.9% | 61.2% | 65.1% | 63.2% |
| Family Medicine | 69.2% | 69.9% | 72.4% | 72.2% | 72.5% | 75.0% | 73.4% |
| Pediatrics | 28.9% | 37.6% | 43.9% | 42.6% | 44.6% | 51.7% | 48.0% |
| Geriatrics | 75.4% | 84.5% | 85.1% | 85.8% | 85.5% | 87.9% | 86.7% |
| Non-Physicians | |||||||
| Clinical Nurse Specialist | 23.9% | 24.9% | 25.8% | 29.9% | 33.3% | 36.4% | 40.7% |
| Nurse Practitioner | 61.6% | 64.9% | 64.7% | 66.3% | 66.6% | 70.8% | 71.5% |
| Physician Assistant | 50.6% | 51.4% | 52.9% | 53.4% | 54.3% | 59.8% | 59.1% |
*Note: the proportions are of allowed charges for all Medicare claims (excluding hospital inpatient, ER, drug and lab)
While the proportion of services that are PCIP eligible is increasing over the observation period, the opposite is true for the proportion of E&M claims (Exhibit 10). Consistent with the decrease in the aggregate number of E&M claims documented above, we observe that the share of E&M claims out of the total Medicare claims is also slightly decreasing over the period. For example, in the case of providers specializing in internal medicine, the share decreased from 41.1 percent in 2005 to 37.5 percent in 2011.
Exhibit 10: Share of PCIP Eligible E&M Claims by Specialty, 2005-2011
| Specialty | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 |
|---|---|---|---|---|---|---|---|
| Physicians | |||||||
| Internal Medicine | 41.1% | 41.1% | 40.1% | 39.3% | 37.3% | 38.3% | 37.5% |
| Family Medicine | 43.2% | 43.0% | 41.9% | 40.9% | 38.6% | 39.2% | 38.4% |
| Pediatrics | 30.9% | 33.8% | 34.7% | 34.7% | 33.0% | 34.2% | 34.1% |
| Geriatrics | 64.8% | 69.6% | 67.7% | 64.1% | 61.0% | 60.0% | 60.3% |
| Non-Physicians | |||||||
| Clinical Nurse Specialist | 27.2% | 26.2% | 25.9% | 27.6% | 28.8% | 30.9% | 32.9% |
| Nurse Practitioner | 55.8% | 56.7% | 54.8% | 51.9% | 48.5% | 50.3% | 50.0% |
| Physician Assistant | 45.5% | 46.1% | 45.0% | 43.8% | 41.0% | 43.4% | 43.1% |
Note: the proportions are calculated out of all Medicare claims (excluding hospital inpatient, ER, drug and lab)
The trends in primary care services and providers discussed above, apply in general to the more restricted sample of PCIP recipients (Exhibits B4-7 in Appendix B). When we limit the number of providers to 2011 PCIP recipients we observe a slight decrease in the average number of eligible claims submitted by physicians
36 For instance, see Stensland et al. 2013.
37 In 2005 almost half of the primary care providers (PCPs) were male, but the share of male PCPs declined to almost 40 percent in 2011 (Exhibit B.1, Appendix B). On the other hand, the share of PCPs aged 55 and above among all male PCPs increased from 24 percent in 2005 to 37.5 percent in 2011 (Exhibit B.1, Appendix B). As observed in Appendix Exhibit B.1, the physician population appears to be aging. The share of male physicians aged 65 and above underwent the largest increase recently, from 18.6 percent in 2010 to 21 percent in 2011 (Exhibit B.9a, Appendix B). A similar increasing trend is also observed among female physicians aged 55 and above (Exhibit B.9b, Appendix B). Finally, in the case of non-physicians, we observe the same steady increase in the share of providers aged 55 and above for both male and female providers (Exhibit B10-11, Appendix B).
38 Source: GAO (2008) – “Primary care Professionals. Recent Supply Trends, Projections, and Valuation of Services “ GAO 08-472T.
We used the provider-level data to address the key research questions related to the Medicare PCIP. We estimated several regression-based models using the DID method to obtain consistent estimates of the PCIP policy effect. 39 In order to implement the DID model, we:
We estimate the following econometric model to identify the effect of Medicare PCIP program on the magnitude of primary care E&M services:

We let be the volume of eligible E&M services provided by provider i in period t; is an indicator variable taking the value of 1 in the years when the PCIP policy is likely to impact the behavior of the providers and 0 otherwise; the vector includes provider characteristics, such as age and gender. The term represents the net influence of random unobserved factors affecting E&M services. Importantly, the estimated coefficient (the coefficient of the interaction term between the treatment group indicator and the post-PCIP policy period indicator) in equation (1) represents an unbiased estimate of the effect of the Medicare primary care incentive payment on the volume of primary care E&M services. The derivation of this estimated effect is presented in Appendix C (C.1). A similar methodology can be applied to estimate the effect of the incentive payment on other outcomes of interest.
The choice of the control group for the DID model was based on several criteria. Ideally, we would have included providers with non-eligible specialties who also supplied E&M services. In order to determine some preferred comparison group providers we:
39 An alternative estimation method is a pre-post analysis, but if there are unobserved factors that affect the magnitude of E&M services supplied by any provider (primary or non-primary care) and the effect of these unobserved factors varies over time, a pre-post model would not yield an unbiased incentive effect.
The estimation of DID regression models is based on the number of eligible providers; the volume of claims for PCIP eligible E&M services and the allowed charges/payments associated with those claims. The volume of E&M claims and payments analyzed here excludes those for hospital inpatient, ER, drug and laboratory services. As we explain above, Medicare providers with a PCIP-eligible specialty (i.e., family practice, internal medicine, geriatrics, pediatrics, NP, PA and clinical nurse specialists) that have at least one Medicare claim are included in the “treatment” group. These are the providers who are likely to be affected by the Medicare PCIP policy. Given that the announcement of the PCIP program was made in 2010, 40 we assumed that the providers with Medicare PCIP eligible specialties would be potentially responsive to the incentive as early as year 2010. Therefore, years 2010 and 2011 represent the post-policy period.
The DID regression models were estimated using several sub-samples: (1) all providers; (2) only providers that appear in all 7 years of data (roughly 44 percent of all providers); (3) providers who were near the PCIP eligibility criteria in 2009 (i.e., restricted to providers who had the share of total Medicare claim payments -- allowed charges-- between 50 percent and 65 percent for PCIP eligible E&M services. About 15 percent of all providers in the sample met this restriction.
In Exhibit 11 we summarize the average volume of PCIP eligible E&M claims and the allowed charges/payments associated with those claims by select patient category and CPT code for providers in the “treatment” group. Comparing the first and last columns, we observe that providers near the 60 percent eligibility threshold generate more E&M claims, on average, compared to the average PCP accepting Medicare (895 vs. 590).
Exhibit 11: Number of PCIP Eligible E&M Claims and Mean Allowed Charges per Provider per Year by Types of Claims for Providers with PCIP Eligible Specialty, 2005-2011
Annual Average Number of PCIP Eligible E&M Claims per provider
Annual Average Allowed Charges for PCIP Eligible E&M Claims per Provider
Note: Summary of PCIP eligibility criteria. Primary care physicians (with internal medicine, family practice, pediatrics and geriatrics specialty) who have at least 60 percent of the practitioner’s allowed charges under the Medicare physician fee schedule (excluding hospital inpatient care and emergency department visits) are eligible for primary care services. The PCIP eligible primary care services are defined by specific E&M codes. Medicare PCIP is also provided to physician assistants, nurse practitioners and clinical nurse specialists who meet the similar eligibility criteria. For the purpose of our analysis we consider the PCPs (with the PCIP eligible specialty) who have 50 percent-65 percent of their services for PCIP eligible E&M services (defined by specific E&M codes) in 2009 are considered to be near the eligibility threshold.
For the control group, the number of providers, the volume of their Medicare claims for E&M services and the associated allowed charges for the providers with the PCIP non-eligible specialties are presented in Exhibit 12. As expected, providers in the control group generated much fewer E&M claims compared to providers in the treatment group. Specifically, providers in the control group supplied less than half the volume of E&M services compared to providers in the treatment group (i.e., 296 vs. 590).
Exhibit 12: Number of PCIP Eligible E&M Claims and Mean Allowed Charges per Provider per Year by Types of Claims for Providers with PCIP Non-Eligible Specialty, 2005-2011
Annual Average Number of PCIP Eligible E&M Claims per Provider
Annual Average Allowed Charges for PCIP Eligible E&M Claims per Provider
40 Source: Patient Protection and Affordable Care Act (‘‘PPACA’’; Public Law 111–148). For our analysis we report a single estimate of PCIP impact under each regression model where year 2010 and 2011 are considered as the post-policy periods. We performed several sensitivity analyses to investigate if the estimated impact is significantly different between 2010 and 2011; we also checked if the results change once we consider 2011 as the only post period. Based on such detailed analysis we did not find any systematic evidence that the estimated impact is different between these two years and they are not sensitive to the choice of post-policy period.
We examined the changes in the number of providers with a Medicare PCIP eligible specialty in a county who have at least one claim for PCIP eligible services to identify the potential impact of the PCIP policy on these providers. Exhibit 13 shows the results from the DID regression models in which we use the number of providers in a county and in a specific year as the outcome variable (Model 1), the number of physicians in each county and year (Model 2); and the number of non-physicians (i.e., NP, PA and CN). The key variable in each model is the interaction between the indicator for PCIP eligible specialty and the indicator for the period after 2009.
In Model 1, the first estimated coefficient suggests that on average the number of Medicare providers with a PCIP eligible specialty and at least one PCIP eligible claim increased by about 2.8 providers per county in each year after 2009 due to the Medicare PCIP. This represents an economically meaningful increase given that on average there were about 15 providers per county per year in a PCIP eligible specialty during the sample period. This increase (almost 19 percent) in the number of providers in PCIP eligible specialties may be the primary reason for the estimated reduction in the number of E&M claims per provider due to the PCIP policy.
In addition, when we restrict the estimation to physicians (Model 2), the increase in the number of physicians with a PCIP eligible specialty attributable to the policy is about 2 per county per year. This is almost 10 percent of the average number of primary care physicians in a given PCIP eligible specialty per county per year (average is almost 19). Furthermore, the estimated policy impact in Model 3 indicates that the number of PCIP eligible non-physicians increased by over 3.6 providers per county per year. Thus, all three models confirm that the introduction of the PCIP policy generated an increase in the number of PCIP eligible providers above and beyond the general increasing time trend. Subsequently, this increased number of providers may have resulted in the reduction in the average number of E&M claims submitted by these Medicare providers after 2009. 41
Exhibit 13: Impact of Medicare PCIP on the Number of PCPs with Medicare Claims for PCIP Eligible Services (2005-2011)
Dependent Variable: Number of Providers per county
PCIP Elig. Specialty Indicator
Elig. Specialty Ind x Post 2009
Median Income ($10k)
Percent in poverty
Percent Population over 65
Note: Robust standard errors are in parentheses; + significance at 10 percent; * significance at 5 percent. The number of observation is based on the number of counties, the number of years, and the number of provider specialties in each model (i.e., physicians include 4 primary care specialties and non-physicians include 3 sub- specialties).
The PCIP policy could impact the number of Medicare providers submitting PCIP eligible claims through several channels. First, the policy may induce an established PCP to start to treat Medicare patients (new or established patient) under PCIP eligible services that they may not have done before. In addition, the policy may also encourage new providers, fresh out of their completion of residency training, to provide PCIP eligible services under Medicare. Lastly, one can also argue that the PCIP policy may encourage providers with a PCIP non-eligible specialty to switch to a PCIP-eligible specialty and increase their chance to receive the incentive payment. This last scenario could be especially relevant for internal medicine sub-specialties such as cardiology, pulmonary disease, nephrology, and endocrinology, which are not PCIP-eligible although the internal medicine specialty is PCIP-eligible. Without judging whether such specialty switching is a desired outcome under the PCIP policy, we first examine to what extent such switching of specialty is prevalent in our dataset; and second, whether such phenomenon is large enough to influence the impact of the PCIP policy on the number of providers who submit at least one Medicare claim under PCIP eligible services.
Based on our 2005-2011 claims data we have estimated that during the post-PCIP policy period (2010 and 2011) there are about 30,864 new primary care physicians (family practice, internal medicine, pediatrics and geriatrics) and 27,927 new primary care non-physicians who have submitted at least one claim under Medicare. (Note that, in this accounting, we do not attempt to distinguish between “new” providers who were induced by the PCIP to participate, and providers that would have entered the Medicare program anyway.) Based on our Medicare data we have estimated that 3,057 physicians with at least one Medicare claim switched their specialty to a PCIP eligible specialty during the post-policy period. Over 50 percent (1,645) of these specialty switches are switches into internal medicine, mainly from internal medicine sub-specialties. The number of specialty switchers is substantially smaller than the number of total new Medicare physicians with a PCIP eligible specialty in the post-policy periods. Thus, switching of specialty could not account for the estimated impact of the PCIP policy on the number of primary care physicians.
Based on our claims data we estimate that during the post-PCIP policy period (2010 and 2011) there are 17,662 new primary care physicians (family practice, internal medicine, pediatrics and geriatrics) who have submitted at least one PCIP eligible claim. Additionally, we have estimated from published sources that during the post policy period there are about 10,000 residency positions filled under primary care, annually, from 2009 to 2011. 42 If the Medicare PCIP policy attracts part of these providers under Medicare to provide PCIP eligible services, then such evidence would be consistent with our estimated impact of the PCIP policy in Exhibit 13.
Exhibit 14 shows the impact of the PCIP policy on the number of providers accepting new Medicare patients (Model 1) and on the number of new Medicare providers (Model 2). The estimated coefficient on the main variable of interest — the interaction between the PCIP eligibility indicator and the post-2009 indicator — suggests that, due to the PCIP policy, on average the number of PCPs accepting new Medicare patients increased by about 1 provider per county per year for a given PCIP eligible specialty. This estimated impact is not negligible given that there are about 9 Medicare PCPs for a given primary care specialty who accept new Medicare patients per county per year during the sample period.
Similarly, Model (2) in Exhibit 14 shows the impact of the PCIP policy on the number of new Medicare providers who have submitted Medicare claims for PCIP eligible services. The estimated coefficient on the main variable of interest suggests that due to the PCIP policy, on average, the number of new Medicare primary care providers with at least one claim submitted for PCIP eligible services increased by 0.148 per county per year for a given PCIP eligible specialty. Given that, on average, there are about 1.4 new Medicare primary care providers per county per year in a PCIP eligible specialty with at least one PCIP eligible claim during the sample period, the estimated impact is again not negligible.
Exhibit 14: Impact of Medicare PCIP on the Number of Providers Accepting New Medicare Patients and the Number of New Primary Care Providers under Medicare with Claims for PCIP Eligible Services (2005-2011)
PCIP Elig. Specialty Indicator
Elig. Specialty Ind x Post 2009
Median Income ($10k)
Percent in poverty
Percent Population over 65
Note: Robust standard errors are in parentheses; + significance at 10 percent; * significance at 5 percent.
41 We have also estimated similar models for the primary care providers who have any Medicare claims (not necessarily under PCIP eligible services) and the estimated effects of the PCIP policy are slightly larger in those cases. These additional results are included in Appendix B Exhibit B 15. In addition we have estimated similar models of providers who met the 60% PCIP eligibility threshold in each year (2005-2011). As expected, the estimated impact of PCIP policy on the number of primary care providers is relatively lower for this restricted set of providers. However, if we focus on this restricted set of providers then we are likely to lose those providers who may have been induced to provide PCIP eligible services in response to the policy, but may not have reached the 60% threshold. Similarly we would lose the information on the providers who have reduced the proportion to below 60%. The estimated results on this restricted set of providers are presented in Appendix B Exhibit B16.
42 Estimates include the following primary care specialties: family practice, internal medicine (including pediatrics), pediatrics. Source: National Resident Matching Program, Results and Data: 2011 Main Residency Match. National Resident Matching Program, Washington, DC. 2011.
The DID estimates from the model using the volume of E&M claims as the outcome variable are presented in Exhibit 15. The estimated coefficient of that interaction term in the first column of Exhibit 15 (i.e., column (1)) indicates that in response to the Medicare PCIP policy PCPs with PCIP eligible specialties reduced their number of PCIP eligible E&M claims by about 52 on average. 43 This represents a reduction in the volume of claims per provider of a little less than 9 percent. Furthermore, we estimate that on average providers with PCIP eligible specialties had about 187 more E&M claims submitted under Medicare during the sample period than the providers with PCIP non-eligible specialties. Also, for the providers with both PCIP eligible and non-eligible specialties the average number of E&M claims submitted went down by 70 claims after 2009.
In addition, we find that as the number of primary care providers per 10,000 population increases, the number of claims per provider decreases. Finally, the volume of claims per provider increases with the provider’s age and with the increase in the size of the Medicare population. The effect of unemployment on the number of E&M claims per provider is also positive and statistically significant.
When the sample is restricted to providers who were near the PCIP eligibility threshold in 2009 (column (3)), the estimated reduction in the number of claims per provider due to the PCIP policy is smaller, only about 33 claims. 44 The reduction in the number of claims per provider in response to the PCIP policy may appear counterintuitive. However, the total number and value of claims may still increase as a result of the policy, as long the number of providers with a PCIP eligible specialty increases at a higher rate than the decline in the number of claims submitted per provider. Thus, a reduction in the number of claims per provider should not be interpreted as evidence of decreased access to primary care services if the number of providers is increasing at the same time.
Exhibit 15: Impact of Medicare PCIP Policy on PCIP Eligible E&M Claims (2005-2011)
Dependent Variable: PCIP Eligible E&M Claims per Provider
Analysis Sample
PCIP Elig. Specialty Indicator
Elig. Specialty Ind x Post 2009